Download the full version of my PhD thesis here or read the summary below!
I defended my thesis on January 19, 2024.
Looking for Interactions: Towards a More Complete Neurocognitive Model of Cannabis Use and Cannabis Use Disorder
This thesis explores the complex nature of cannabis use, including factors that influence initiation, escalation towards heavy use, and the potential development of a cannabis use disorder (CUD). The changing legal landscape and increasing availability of cannabis have contributed to a decrease in perceived harm and an upsurge in usage. The prevalence of cannabis use is high worldwide and the rise in the delta-9-tetrahydrocannabinol (THC) to cannabidiol (CBD) ratio, with increasing THC levels and decreasing CBD levels, may amplify the potential harms of cannabis use.
While cannabis initiation is common in all age groups, most individuals initiate cannabis use during adolescence (UNODC, 2019) and the prevalence of cannabis use peaks during young adulthood (e.g. 26.4% of the 20-24 year old Dutch; Trimbos-instituut & WODC, 2021). Approximately 10% of cannabis initiators become daily users, but the factors driving escalation are not fully understood. Cultural attitudes, social environment, limited behavioral control, individual motivations for use, and sex or gender differences all contribute to the effects of cannabis use and the development of a cannabis use disorder (CUD).
CUD is one of the most prevalent substance use disorder characterized by problematic cannabis use that impairs functioning or causes distress. The direct effects of THC on the endocannabinoid system and the release of dopamine in the brain’s reward pathway are thought contribute to CUD. Associative learning processes also heighten the significance of drug-related cues, leading to compulsive use and withdrawal symptoms upon cessation. Importantly, not all daily cannabis users develop CUD, highlighting the need to comprehend individual differences in usage patterns and potential negative consequences of heavy use. Heavy cannabis use and dependence can result in altered brain processes associated with cognitive control and motivation. Individuals with CUD may also exhibit altered activation patterns in various brain regions during tasks involving attention, interference control, and working memory. However, the causal relationships and long-term effects of these brain changes remain incompletely understood.
The thesis aims to investigate the complex interactions between internal and external factors influencing cannabis use trajectories and consequences of use. This includes examining brain functioning, cognition, motivation, sex/gender, mental health, drug cues and attentional bias, region, cultural attitudes, COVID-19, and social factors. By studying these factors, the goal of this thesis is to move towards a more complete neurocognitive model of cannabis use and dependence that can inform prevention, intervention, and policy.
Results Summary
Chapter 2, aimed to summarize and evaluate knowledge of the relationship between heavy cannabis use, CUD, and the Brain, discussing epidemiology, clinical representations, potential causal mechanisms, assessment and treatment, as well of prognoses. Heavy use and CUD appeared to be consistently associated with learning and memory impairments – which might resolve after prolonged abstinence – and comorbid psychiatric disorders are common is heavy users and those with CUD. Evidence regarding other cognitive domains and neurological consequences is limited or inconsistent. Treatment results in abstinence in only a minority of patients, but treatments aiming for reduction of use appear more successful. The impact of heavy use and CUD on brain outcomes appears to depend on age of onset of use, heaviness and frequency of use, CUD severity, psychiatric comorbidity, as well as THC/CBD ratio. Specifically focussing on evaluating the recent evidence for short-term and long-term effects of cannabis use on cognition, Chapter 3 found cannabis intoxication to be associated with impaired learning and memory, attentional control and motor inhibition. Evidence regarding the long-term effects of heavy use is less consistent, with impairments most constantly observed for learning and memory, attentional control and the presence of attentional bias towards cannabis cues. Studies of the effects of cannabis on cognition are hampered by difficulties measuring cannabis exposure, the lack of control over sub-acute effects, the incomparability of included cognitive measures, and the large variety of included samples.
Chapter 4 aimed to assess how hair-derived cannabinoid concentrations – offering insight into three-month cumulative exposure – were associated with common self-report measures of cannabis use and cannabis use-related problems (N=74, near-daily cannabis users with CUD). THC was detectable in over 95% of the hair sample of individuals that tested positive for THC on a urine test, supporting the potential for of hair for detecting cannabinoids. However, THC, CBD, and THC/CBD concentrations were not associated with self-reported use and use-related problems, indicating limited utility for quantification of use. THC concentrations were associated with self-reported measures of potency, but additional research is needed to assess the utility of these self-reported potency measures as an indicator of THC concentrations in a wider sample of users. Importantly, research comparing hair-derived cannabinoid concentrations with other biological matrices of use (e.g. plasma) and self-report measures of use is crucial to evaluate and confirm the validity of hair analyses for quantification of cannabis use.
As cannabis use in women is increasing worldwide but research assessing gender differences in cannabis use and CUD is lacking, Chapter 5 assessed gender differences in CUD symptoms using a network analysis approach (Weekly cannabis users; N=1257, Men: N = 745, Women: N = 512). This approach allows for the assessment of interactions between different CUD symptoms which could well be crucial in the etiology of CUD. Looking at the prevalence of symptom endorsement, men more often reported 6 out of 11 symptoms than women, while total CUD scores were similar (mean difference < 1 symptom). However, the symptom network structure, strength, and centrality did not differ between men and women. When considering the presence of mood and anxiety disorders in the model, gender differences did appear. In men, mood disorder presence was only associated to the presence of anxiety disorders, which in turn was associated with the CUD symptom network through unsuccessful attempts to reduce or quit, which could increase anxiety but also be increased by anxiety (i.e., possible feedback loop). In women, the presence of anxiety disorders was only associated to the presence of mood disorder, which in turn was associated with the CUD symptom network through craving and withdrawal, indicating a potential women-specific self-medication loop. These results highlight the complexity of symptom interactions and the potential gender differences in how comorbid psychiatric disorders are associated with CUD.
Chapter 6 assessed sex differences in cognitive control related brain processes that might underly CUD, using an N-back working memory (WM) task performed inside an MRI scanner (N=189, frequent cannabis users: N = 104 (63% men), controls: N = 85 (53% men). Task performance was lower in the cannabis group when the task got at its most difficult. MRI results indicated a relatively smaller reduction in WM-related activity in the precuneus and posterior cingulate cortex at higher WM load, indicating a relative over recruitment of default mode related regions in cannabis users when cognitive demand increased. Sex differences were only observed in exploratory analyses within the cannabis group: men showed higher WM-related activity in the superior frontal gyrus compared to women. Differences in brain activity were not directly associated with performance differences and further research is needed to assess whether altered brain activation might be associated with performance when cognitive load is increased further.
Chapter 7 aimed to increase this cognitive load by adding distracting cannabis-related and neutral flankers to the N-back working memory task (N=69, near-daily cannabis users: N = 36, controls: N = 33). These cannabis-related flankers specifically were expected to cause interference in the cannabis users, reducing performance and affecting brain activity. The flanker presence did not affect performance, but in cannabis users compared to controls, the presence of cannabis flankers was associated with reduced WM-load related activity in the insula, thalamus, superior parietal lobe, and supramarginal gyrus. These results could indicate that the presence of cannabis cues can interfere with cognition related brain processes in cannabis users, especially when cognitive demand increases.
Heavy cannabis use has also been associated to attentional bias towards cannabis stimuli. Using the same words as presented as flankers in chapter 7 as stimuli in a cannabis Stroop task, chapter 8 assessed the presence of attentional bias in cannabis users with different levels of use and CUD severity (N=560, 71% men). Only those is treatment for CUD showed an attentional bias towards cannabis stimuli and group differences were only observed when comparing those in treatment for CUD with those that never-sporadically used cannabis. Furthermore, the association between attentional bias and craving in their association with cannabis use and related problems was assessed in occasional and regular users (N=358). Average craving during the test session mediated the association between attentional bias and cannabis use as well as cannabis-related problems. The expected moderating effects of interference control on these associations were not observed, but interference control was directly associated with heaviness of cannabis use, indicating potential sub-acute effects of use on control related processes.
Changes in cannabis legislation have been paralleled with reductions in the perceived harm of cannabis use, which has been associated with increased initiation and persistent use. Perceived harms and benefits exist on the personal level, friend and family level, as well as regional (state or country) level, affecting the experienced cannabis culture. Cultural neuroscience research has shown that culture can affect a variety of brain processes underlying our daily life behaviors, but this has not been explored regarding the brain processes underlying cannabis use. Chapter 9 assessed the associations between cultural attitudes towards cannabis use and resting state functional connectivity (RSFC) in three brain networks regularly associated with substance use: the default mode network, executive control network and salience network (N = 189, near-daily cannabis users with CUD: N = 110, controls: N = 79). Cannabis users showed lower RSFC than controls within the dorsal salience network, with this lower RSFC being associated with higher cannabis use in the cannabis group. Furthermore, cultural attitudes – from all three perspectives – moderated several associations of cannabis use, CUD symptoms, and cannabis use related problems with RSFC within the default mode network, executive control network, and salience network. Looking at RSFC between these networks, no group differences were observed. However, personal perceived benefits and perceived harms on the country/state level moderated the association between CUD symptoms and RSFC of ventral and dorsal default mode network regions. While these complex interactions have unknown clinical utility at this stage, it highlights the importance of considering individual differences in cannabis culture in the association between measures of cannabis use, use related problems, and brain functioning.
Chapter 10 then explored how cultural attitudes as well as site differences – Texas, USA and The Netherlands – might moderate the association between cognitive control related brain activity and cannabis use, CUD symptoms, and cannabis use related problems, using an N-back working memory task (NL participants: near-daily cannabis users with CUD: N = 60, controls: N = 52; US participants: near-daily cannabis users with CUD: N = 40, controls: N = 32). Looking at cannabis attitudes, cannabis users were more positive and less negative than controls from both the personal and perceived friend-family’s perspective. US cannabis users were even more positive and less negative than the NL participants. Although legislation differences are large, there were no site differences in perceived country-state attitudes. MRI results showed that cannabis users from TX – compared to NL users – and those cannabis users that perceived more positive country-state attitudes, displayed stronger positive associations between grams/week and WM-related activity in the superior parietal lobe. On the other hand, cannabis users from NL – compared to TX users – and those cannabis users with less positive personal attitudes, showed stronger positive associations between gram/week and WM-load-related activity in the temporal pole. These results indicate that both site differences and individual differences in attitudes towards cannabis use moderate associations between heaviness of use – but not cannabis use related problems and CUD severity – and WM- and WM-load related brain activity. Interestingly, differences in legislation did not align with the perceived harms and benefits of cannabis use in individuals from Texas (USA) or The Netherlands, and site and individual perceptions appeared to be differentially associated with the association between cannabis use and control related brain activity.
Cultural factors are not the only external factors that can affect cannabis use: a variety of life changes can heavily impact cannabis use and the development of CUD. One of the biggest life changing events in the last decades has been the COVID-19 pandemic and the associated lockdown. In chapter 11 we aimed to assess the influence of the first Dutch COVID-19 lockdown on cannabis use and CUD and to evaluate the role of changes in mental health and psychosocial stressors therein (N=183, monthly-daily cannabis users: N = 120, non-using controls: N = 63). Results showed that the lockdown was associated with an increase in cannabis use, but not CUD severity. Furthermore, cannabis users showed increased loneliness, but improved contact with partners and family, which was similar to results in controls. On average, mental health was not affected. However, individual differences in severity of use before the lockdown, COVID-19 related worries, changes in anxiety, changes in use motives, and contact with family explained unique variance in changes in cannabis use or CUD during the lockdown.
Aside from changes in the social environment, social influence is also known to be associated with substance use. The social plasticity hypothesis suggests that social attunement – the adaptation to and harmonization with one’s environment in the absence of group pressure and conformity motives – plays an important role in the risk for developing alcohol use disorders (AUDs) during adolescence, whereas in adulthood it paradoxically may make individuals more sensitive to the social pull to reduce drinking. Chapter 12 described the development and validation of the 11-item Dutch social attunement questionnaire, including two subscales of social attunement cognition and social attunement behavior (N = 576, exploratory factor analysis: N = 373, confirmatory factor analysis: N = 203), showing acceptable internal consistency and good measurement invariance to gender. Exploratory assessment of the role of social attunement in alcohol use behavior showed that social attunement explained additional variance in the association of age and perceived peer drinking with alcohol use. Further research is required to assess the utility of the social attunement questionnaire in a broader variety of social settings, including social cannabis use.
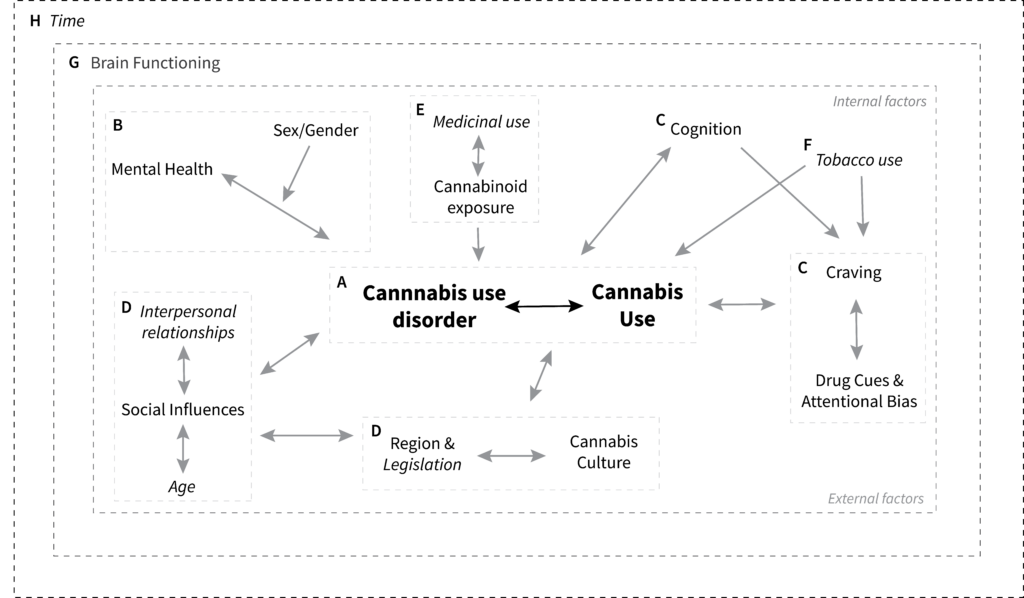
Figure 1. Initial neurocognitive model of cannabis use and CUD. Letters indicate different highlight themes and challenges for future research as discussed in this chapter. Grey lines represent the – often potentially bidirectional – associations that are crucial for future research to explore. The italic items represent novel factors that – although not directly assessed in my studies – appear to be important additions to this model. Additional layers have been added to indicate the overarching importance of brain functioning in the etiology of cannabis use and CUD and the importance of assessing those processes over time to assess developmental processes and causality.
Discussion & Conclusion
The multimethod studies presented in this thesis can be a start to build towards a more complete neurocognitive model of cannabis use and CUD (Figure 1). First, our studies highlight the importance of differentiating between heavy use and dependence – which most studies to date fail to do – as they differentially associate with cognition and brain functioning (Figure 1-A). Second, studies should embrace and assess the presence of comorbid mental health problems in those with CUD and consider potential interactions with gender therein (Figure 1-B). Third, studies should aim to include measures of motivation and control processes to test the theoretical importance of their interactions in cannabis use and CUD (Figure 1-C). Fourth, social and cultural factors are regularly ignored even though changes in the social environment, social use, and cultural attitudes towards use might be important drivers of initiation, continuation, and escalation of use (Figure 1-D). Studies should focus on developing and validating measures that assess these factors and include them in studies on cannabis use across the lifespan as the influence of these factors could be partially age dependent. Fifth, medical cannabis use is increasing, but evidence for its utility – especially as a treatment of mental health symptoms – is limited (Figure 1-E). It is crucial for studies to assess use motives – at least differentiating between primarily medical and recreational motives – to provide additional evidence for the risks and benefits of use. Furthermore, the measurement of cannabinoid exposure should be encouraged to start differentiating the effects of cannabinoid exposure, amount of use, and use related problems. Sixth, tobacco use remains one of the biggest challenges in cannabis research, particularly in Europe where combined use is very common (Figure 1-F). It is crucial to collect information on tobacco use with as much detail as is feasible (preferably using timeline follow-up measures) and to separate combined use from sequential use to help us understand the interactions between nicotine and cannabis.
The interactions described above are all fundamentally associated to brain functioning, but increasingly complex interactions make it difficult to assess the clinical implications of measures of brain functioning. It remains crucial to assess brain functioning as one of the fundamental factors underlying behavior (Figure 1-G) but assessing interactions between behavioral outcomes to inform prevention and treatment outcomes should be prioritized to reduce harm. Finally, we have limited understanding of causality and the development of these interactions over time. As the use of experimental designs is inherently limited by ethical constraints in the addiction field, it remains important to invest in studies assessing the effects of time on both the short (e.g. experience sampling methods) and longer time scale (e.g. multi-year cohort and longitudinal designs).
Together, these findings offer valuable but incremental contributions that can help to steer future research in the direction of developing a more comprehensive neurocognitive framework for understanding cannabis use and CUD. However, in order to achieve this objective, it is crucial to prioritize measurement: we must strive towards a consensus on the essential assessments required in cannabis research. Drawing from my experience in conducting multimethod cross-cultural studies on cannabis use, I propose a starting point for the discussion in reaching this consensus. Figure 2 presents a cannabis research checklist that includes measurements I believe should be consistently incorporated in cannabis research, as well as additional measures that should be considered based on study goals, budgetary constraints, and time limitations. Extending these measurement standards beyond the mere measurement of cannabis use and cannabis use disorder can facilitate study comparison and prompt researchers to move beyond examining group differences, considering individual variations as well.
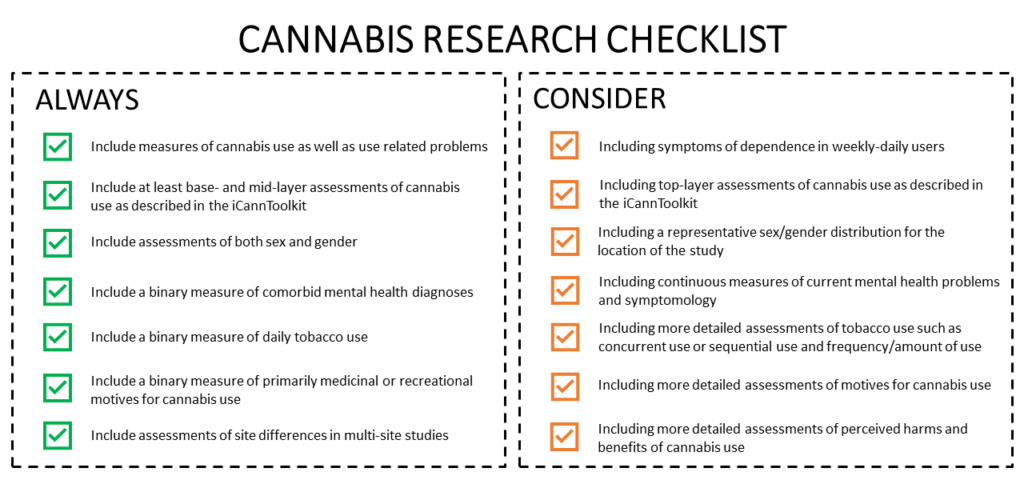
Figure 2. Cannabis Research Checklist. A proposal for a comprehensive field-wide cannabis research checklist, including measurements that should always be included to increase comparability of studies and measurements that should be considered based on the goals, budget, and time constraints of the study.